Notes on My Chemotherapy
2021-02-04
Nobody likes an addendum.
Appendices are great (ask any Tolkien fan). P.S.'s are the best (especially if they're from a penpal).
But addendums. Nope. They change the rules, after you've started playing. After the game's over, even.
I recently got dropped with this whopper of an addendum:
Orcein stains performed on blocks A3 and A5 highlight elastic fibers
wrapping around nests of tumor cells, consistent with vascular invasion
A lil' background
Previously, on "Halt and Catch Cancer", I thought I was in the clear. Sure, I'd been diagnosed with Stage II colon cancer at age 34. But the neato robotic surgery to remove my sigmoid colon (and my grisly barnacle of a tumor) was successful, with no signs of the cancer spreading to the nearby lymph nodes (which are essentially the Information Superhighway of your body's immune system).
Officially, we're talking a PT3N0 pathology, where N means the number of lymph nodes with tumor cells (zero, in my case, of the 21 that were removed and inspected) and T means the levels of colon wall that the tumor "broke through." N0 is awesome and T3 is not-so-awesome. My tumor was pretty darn close to breaking through the colon wall. But the fact that I had no lymph nodes affected was a good sign -- a good enough sign that no chemotheraphy was being recommended by my USCF doctor crew.
Now, after my blog post on this whole "cancer sitch," I'd been in touch with friends and other wood-workers who were, unfortunately, familiar with this process. One, in particular, has been highly tuned into the research and literature around colon cancer, and he pushed me to make sure I fully understood my pathology. He also mentioned that he's seen folks with my PT3N0 pathology do chemotherapy on a preventative basis. Given that my big missive in my last post was about "becoming your own health advocate," his advice hit hard, because I was already lapsing in my attentiveness. Frankly, I was exhausted from the surgery, relieved by the results, ready to move on, and the pathology report itself was confusing af.
Actually, you know what? I'm just going to paste it here:
FINAL PATHOLOGIC DIAGNOSIS
Sigmoid colon, sigmoid colectomy:
1. Adenocarcinoma, moderately-differentiated, invasive through
muscularis propria into pericolic adipose tissue, negative margins; see
comment.
2. No tumor in twenty-one lymph nodes (0/21).
COMMENT:
COLON CARCINOMA SYNOPTIC COMMENT
- Procedure: Sigmoid colectomy.
Result Information
All Reviewers List
Pathology PDF Report
Narrative & Impression
Harrington, Charles
- Location of tumor: Sigmoid colon.
- Tumor size: 3.3 x 2.5 x 1 cm.
- Macroscopic tumor perforation: Not identified.
- Histologic Type: Adenocarcinoma.
- Histologic Grade: Moderately-differentiated (low grade).
- Microscopic depth of invasion: Tumor invades through the muscularis
propria into pericolic soft tissue (pT3).
- Margins: Negative.
- Proximal margin: Negative (tumor is > 4 cm from margin).
- Distal margin: Negative (tumor is > 4 cm from margin).
- Circumferential (radial) margin: Negative (tumor is > 3 cm from
margin).
- Treatment effect (modified Ryan score, scale 0-3): No known
presurgical therapy.
- Lymphovascular invasion: Not identified on H&E (orcein stains will
be performed on blocks A3 and A5, and the results will be reported as an
addendum).
- Perineural invasion: None.
- Tumor Deposits: Not identified.
- Lymph node status: Negative (number of lymph nodes examined: 21).
- Other pathologic findings: None identified.
- AJCC Pathologic Stage: pT3N0.
- Ancillary studies: Immunohistochemistry for DNA mismatch repair
proteins will be reported in an addendum.
Addendum Comment
Immunohistochemistry was performed to evaluate the status of DNA
mismatch repair protein expression on block A3. The results in the tumor
cell nuclei are:
MLH1 expression: Present.
PMS2 expression: Present.
MSH2 expression: Present.
MSH6 expression: Present.
Expression for all four markers, in most cases, indicates that the DNA
mismatch repair proteins are intact. This result should be correlated
with the clinical presentation and family history to determine the need
for further work up for Lynch syndrome
Probably TMI, but this will actually be easier for me to find later, instead of spelunking through the oh-so-painful EPIC MyChart software. Am I allowed to share this? I DON'T KNOW AND I DON'T CARE.
As you can see, this plaintext nightmare is full of strange and wonderous medical terms. Yes, the doctors walk you through it but still... it's a lot. I did push them to explain the terms, like what negative margins mean and why they're a good thing, although I kind of forget already so I won't try to explain.
After this walk-through with the docs, I felt good about my plan. No chemo needed. Just ongoing tests and CT scans and blood work and colonoscopies over the next five years to make sure that the cancer wasn't back, led by the UCSF Cancer Survivorship Clinic. Sure, that wasn't nothing, but it also isn't that bad, considering how lucky I am to have caught this thing and gotten it removed ASAP. The idea was, after five years, I'd be back in the general population for risk of colon cancer. Cured.
But then, during my first Survivorship Clinic convo in November, I recalled that one line from the pathology... the one mentioning the addendum that I hadn't yet seen. I ask about it. We dig in, and we find this:
Addendum Comment
Orcein stains performed on blocks A3 and A5 highlight elastic fibers
wrapping around nests of tumor cells, consistent with vascular invasion
Consistent with vascular invasion. Welp, that can't be good.
At this point, I'm immediately whisked off the UCSF Oncology Department.
New faces and new tests and new plans
A hospital is a series of interconnected rings, all slightly Venn Diagramming each other, kind of like the Olympics logo. As a patient, you tend to orbit one of the rings. But sometimes you'll Three Body Problem your way over to another ring.
In my entire diagnosis and surgery process, I'd never made it over to the Oncology (aka cancer) ring -- I was stuck in Surgery World. But, after this addendum, I'm now squarely in their circle.
So, what's our goal now? Well, now that we've noticed that my cancer has slightly spread into the vascular system, we need to figure out what to do about it. First, let's remember the good stuff - the rest of the pathology is relatively awesome. Next, let's get some more data!
We do these tests:
- Signatera - looks in your blood for tumor cells
- Oncotype - looks at your tumor and rates the likelihood of recurrence
Let me reiterate that my explanations of these tests (and anything medical-related) is entirely my random-dudeman-laymen's explanation. I hope to provide one person's context and interpretation of these confusing and scary things. I'm open to feedback and information on what I can do better.
Insurance aside
Insurance didn't want to cover the Oncotype test, because, of course. Insurance doesn't want to cover a lot of things, especially brand new "cutting edge" stuff, like the Oncotype test.
Instead, insurance wants to make sure that you really-super-duper-need whatever it is they're going to give you, to the point where there's basically no way they can say no. My doctors have been amazing advocates for me, helping make sure that insurance knows how important these tests and treatments are for my health. THANK YOU, UCSF.
Insurance is frustrating and scary. I do not understand it. I do not want to understand it. I wish it was simpler. I wish I didn't have to make sure that I was "covered" for things related to my health and my family's health. I also know that I'm incredibly lucky to have good insurance. I took a screenshot from my insurance app back in December:
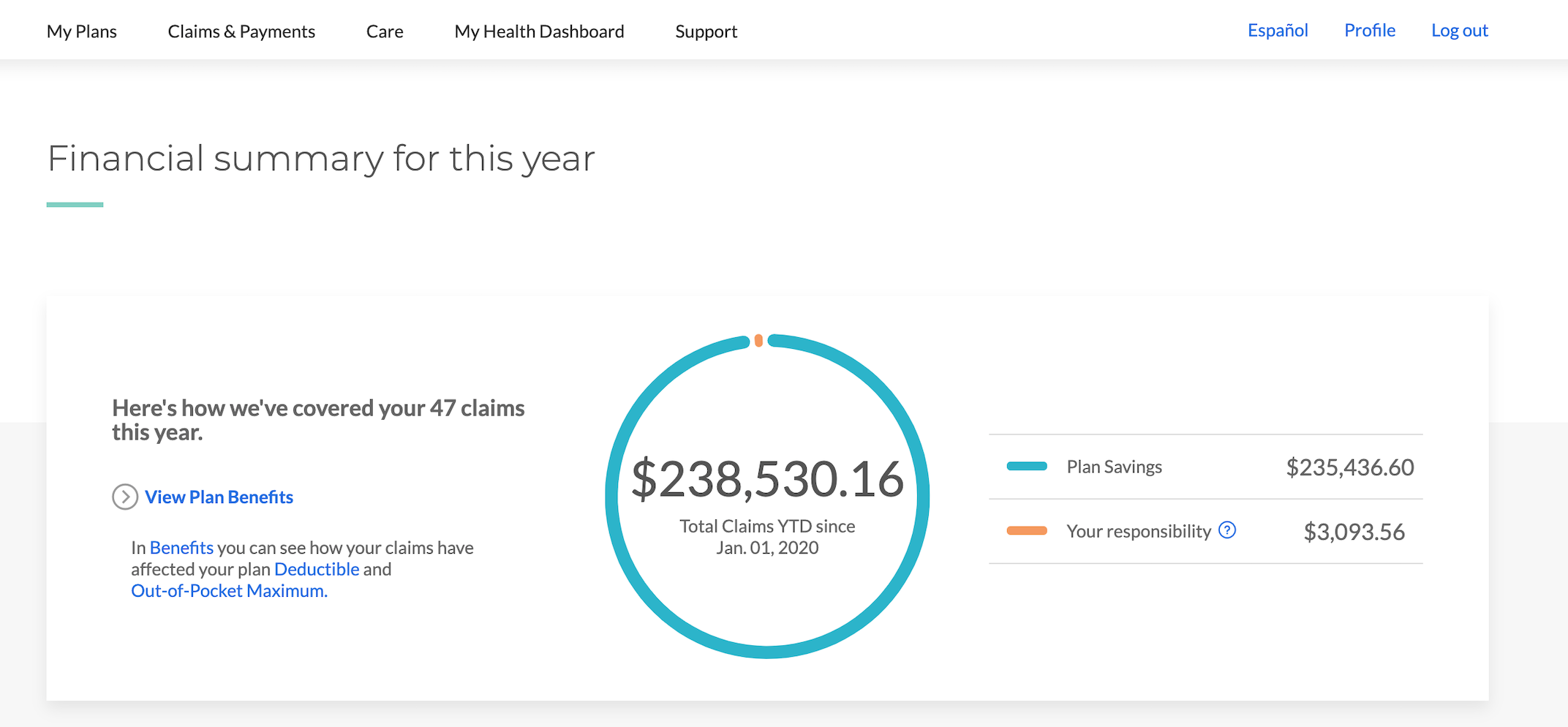
WTF. That's an insane amount of money. But my life was saved, sooo...? The insurance company even assigned me a nurse to "check in on me" as a resource back in November and December, which sadly was more of a nuisance than anything else. And, then, when my company switched insurance providers at the beginning of 2021, this nurse service stopped abruptly. The whole thing's odd. But I can say again that I am extremely grateful to have had good insurance during my cancer treatment.
Make a new plan
The Signatera is clear, which is great. No circulating tumor cells in my blood. I ask the question, "Doesn't this mean I'm, like, good for life now?" And apparently no. They can't say that. They can only say, "We don't see anything right now." It's the balance sheet of cancer. Just cause things look good right now doesn't mean that next year or next quarter's gonna be the same. Past performance is no indication of future something-something.
Oncotype's pretty good, too. From what the doc explains, this test suggests that my tumor has a 12% recurrence rate. This is a low number and I should be happy about it. And I am. But I want it to be zero, obviously. Also, recurrence isn't talking about new polyps growing in my butt and starting cancers -- that can still happen. Recurrence is about whether cells from my now-removed cancer tumor are going rear their awful heads again, somewhere else in my body.
It's at this point that we get into the discussion around chemo. There's evidence that chemo can help reduce the recurrence rate even further. My oncology team brings my data to this cool-sounding UCSF "Tumor Board" meeting, and they advise a chemo treatment. The evidence suggests that we can bring down my recurrance rate from 12% to 6%.
But they also reiterate that it's my choice. I can say no. As my aforementioned friend said, "You don't do chemo recreationally." In fact, the doctors explain that if I were an old man, they might not advise treatment. But since I'm young and restless, it makes more sense for me to do whatever I can to improve my chances.
Duh, let's do this thing.
So, what's chemotherapy like?
Well, first of all, there's all different kinds of chemo. I didn't know that. I'm on a combo colloquially called CAPEOX (which I thought sounded a bit like a rival Star Fox gang). It stands for capecitabine (brand name is Xeloda) and oxaliplatin. Cape comes in pills and ox is an IV drip.
But wait -- more decisions. Do we do six months or three months of treatment? We review the data from a Japanese study, and we conclude that there's no measurable difference, so we go with 3 months, due to risk of chemo side effects.
Chemo is not a pure function
Chemo has side effects. Here are the things that I've encountered so far:
- super cold fingers and toes
- lockjaw when I start eating
- clenching claw hands
- it hurts to cry (and I just finished the last season of Halt and Catch Fire, so yeah..)
- no appetite, not even for pizza or beer
- nausea
- kinda a sad feeling
- dead sperm(!)
Shockingly, there's no hair loss expected. I'm already in a thinning situation "up there," but it's not supposed to get any worse. A small, dumb part of me thinks that once treatment's over that it might even get better! But this small part is very dumb.
Let's talk about the sperm stuff. As a result of doing chemo, there's a good chance that my swimmers are gonna be dead for good. There's also a chance that they can come back. But, if I want to ensure that Carly and I can have the family we want, I need to do sperm banking, quickly! Apparently, there's a ticking clock on starting chemo post-surgery (something like within 8 weeks). So, I've got a week to do as much sperm banking as I can! Fun!
The sperm banking process is hilarious. You go to a building, then into a waiting room, then you are led to a tiny little room with a metal door in the wall. When you are done collecting your sample in a cup, you open the door in the wall and put the cup in there, and then press a button, and someone on the other side grabs it. In between that, there's literally a Roku porn subscription and a big TV. I went four times in a week. We got some good stuff collected.
Another note on the 3 months vs 6 months decision - there are other potential side effects to chemo that factor into the timing decision. The big one in my case is something called neuropathy. Essentially, chemo can potentially cause long-term, life-altering nerve damage. The signs of it often begin with numb feet and hands, which I will admit seem rather easy to confuse with the expected, but not serious symptoms of cold hands and feet. The docs explain that any signs of neuropathy need to be reported immediately and we will halt chemo immediately, because the long-term negative effect of neuropathy far outweighs the gains in any reduction of recurrence rates in my case.
Now, given of all that prep and preamble, it's finally time to start chemo!
Charlie the Cyborg
Wait. We need a way to get the chemo into your body. There's two options: a PICC line or a port. In either case, we need a tube that's threaded through your veins directly above your heart. If you go PICC, we gotta thread that in for every single treatment. If you go port, you only do that once, but you get this Tony Stark metal disk thing in your chest. You can guess which one I chose.

Now I have an ID card that explains why metal detectors don't like me anymore.

Gross and weird, but also cool and weird. With this port, it's a simple little pin prick to get me all connected to the IV stuff. Here I am plugged in.

My three week cycle consists of this:
- Day One: Ox drip and start taking pills
- Next 2 weeks: pills 2x a day
- Third week: Nothing
Then, start over, for 4 times total.
The point of the third week is to help your white blood cells recover. The chemo fries them, too. It basically kills anything fast growing in your body (my interpretation!), so your useful blood cells (and sperm and hair etc etc) are impacted. Not a super great thing to happen during a global pandemic, weakening your immune system and all.
The drip takes like 2 hours. I usually bring some books and a chicken parm sub and my Nintendo Switch. Here's me after a pee-break:

I buy this pill box on Amazon, cause why not:

This sucker lives in our kitchen counter in plain sight so that I never forget to take my 2x a day sets, and so far, I haven't ever forgotten.
What next?
This has been a long, strange trip of a six-month period. I'm currently in the second week of the third cycle. My third cycle had to be pushed back a week because my white blood cells were too low. I came back the next week, and they were still low, but we decided to proceed, and just dropped my cape dosage from 2000mg to 1500mg (3 pills 2x a day instead of 4 pills 2x a day). In another week, I get to have the glorious "week off" (when I again crave the taste of beer), and then we're back for the fourth and final round.
I can't wait for this to be over. I can't wait for this port to be out of my chest. I'm happy that I'm doing everything I can to ensure that I have a long and healthy life. I'm eager to get back on the UCSF Survivorship Clinic plan, and start improving my diet to reduce inflammation (and all this other stuff that's supposed to help prevent cancer).
I have learned a lot about cancer and health. My heart breaks when I think about children who've suffered from cancer. My infusion center is the adult center. I'm not sure I could stomach seeing children and babies getting chemo. I'm crying right now even thinking about it (which hurts, if you remember my side effects). Cancer is terrible and it can affect anyone. This is where I re-impart my advice about being your own health advocate.
Thanks to Carly and my family and friends and work peeps for your love and support.
Fuck cancer. Create wonderful things, be good, and have fun.